Laser Frenectomy
Frenectomy—the surgical removal of the oral frenulum—has advanced tremendously with the
introduction of diode laser technology. This innovative method
offers unmatched precision, minimal discomfort, and a rapid recovery compared to traditional
techniques.
It’s effective for treating both a short lingual frenulum (commonly known as tongue-tie) and an
abnormally attached labial frenulum. In fact, the laser
not only minimizes bleeding, swelling, and pain but also disinfects the surgical site, thereby
reducing infection risks and speeding up healing. These
benefits make it an excellent choice for patients of all ages.
In this article, we explore the clinical applications of diode laser technology in both lingual
and labial frenectomy. We compare it with conventional
methods to highlight its many advantages in modern dental practice.
What is the Frenectomy?
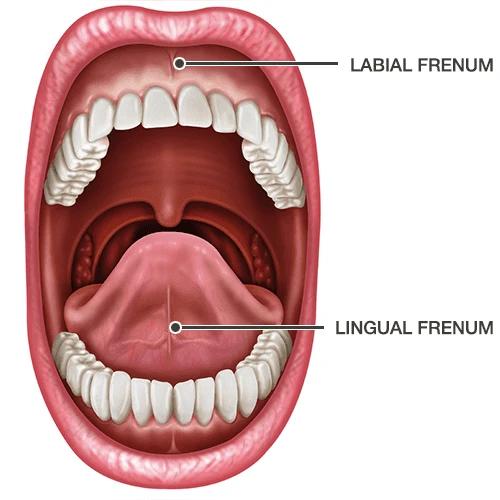
Lingual frenectomy is a treatment that involves surgically—or using laser technology—severing the lingual frenulum, the band of fibrous tissue that connects the underside of the tongue to the floor of the mouth, to correct its shortened condition. Ankyloglossia, commonly known as tongue-tie, can cause a range of issues. In infants, it may lead to breastfeeding difficulties; in children, it often results in speech problems such as unclear pronunciation of retroflex sounds; and in adults, it can limit effective chewing.
According to the Journal of Oral and Maxillofacial Surgery Clinical Guidelines, approximately 4%–10% of newborns have tongue-tie, and nearly 30% of these cases require surgical intervention to restore proper tongue mobility. Clinical indications include tongue-tie that leads to feeding challenges in infants, speech impairments in children, and compromised masticatory function in adults.
Clinical indications include:
- Infants experiencing breastfeeding difficulties due to tongue-tie.
- Children with speech impairments, such as unclear pronunciation of certain sounds.
- Adults facing limitations in chewing function.
Labial frenectomy removes a low-attached labial frenulum. This mucosal fold connects the lip to the gingiva. The surgery fixes a wide gap between the front teeth (diastema) caused by the frenulum’s pull. Research shows that abnormal frenulum attachment is a common cause of incisor spacing during the mixed dentition period (ages 6–12). It accounts for 15%–20% of cases. The ideal time for surgery is late in the mixed dentition period, around age 10. At this stage, children are more cooperative and the alveolar bone is stable. This timing can help prevent permanent malocclusion.
Why Choose Diode Laser for Frenectomy
Diode lasers offer significant advantages in oral frenectomy, including both lingual and labial procedures. Their minimally invasive nature, precision, and fast recovery have been validated by multiple clinical studies.
1. Minimally Invasive
Diode lasers use a high-energy beam to precisely target tissue, eliminating the need for large incisions or sutures required in traditional surgery. This significantly reduces damage to surrounding healthy tissue.
For example, a randomized controlled study on 40 cases of labial frenulum revision showed that the laser group only required contact fiber cutting, with no need for sutures post-operation. In contrast, the traditional group underwent incision and suturing, resulting in a larger wound area.
Additionally, the laser’s “non-contact” mode, especially for non-vascular lesions, further minimizes mechanical trauma risks.
2. Reduced Bleeding and Swelling
Diode lasers, with wavelengths ranging from 810–980 nm, are highly absorbed by hemoglobin. This allows the laser to simultaneously seal blood and lymphatic vessels through photothermal effects, significantly reducing intraoperative bleeding.
Clinical data show that in laser procedures, the average blood loss is less than 5 ml. In contrast, traditional surgery requires hemostatic forceps and suturing, leading to increased bleeding and additional hemostatic interventions.
Regarding postoperative swelling, the laser’s biostimulatory effect helps reduce inflammation by lowering the release of inflammatory factors such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), effectively minimizing edema.
3. Faster Healing Time
The laser’s precise cutting and sterilization effect reduce the risk of postoperative infection. Additionally, its low-energy bioregulatory function accelerates tissue repair.
A comparative study found that complete wound healing took 9.8 ± 0.4 days in the laser group, compared to 6.9 ± 0.4 days in the traditional group. Although the laser group had a slightly longer healing time, their postoperative pain score (VAS) was 40% lower within the first three days, significantly improving patient comfort.
For pediatric patients, laser treatment eliminates the need for sutures and causes minimal pain, often shortening the recovery period to less than seven days.
4.Enhanced Precision
Diode lasers allow millimeter-level cutting precision by adjusting power output (typically 1.5–3W) and fiber diameter (200–400μm). This makes them ideal for delicate anatomical areas, such as short lingual frenulum or abnormally attached labial frenulum.
For example, in high labial frenulum excision in children, a 980nm laser can precisely remove abnormal attachments without damaging nearby alveolar bone or nerves. Furthermore, the laser’s real-time coagulation function keeps the surgical field clear, reducing the risk of errors.
Clinical Procedure of Diode Laser Frenectomy
Before surgery, patients should undergo a thorough evaluation. The surgical area is disinfected, and a 2% lidocaine topical anesthetic gel is applied for surface anesthesia.
For the procedure, 450nm blue light is recommended over the traditional 980nm laser due to several advantages:
- Higher Absorption Rate – The 450nm wavelength is more efficiently absorbed by hemoglobin and pigments than 980nm, enabling effective cutting and coagulation at lower power settings.
- Lower Heat Diffusion – It provides precise, localized action, reducing thermal damage to surrounding tissues. This helps maintain clean incision edges and promotes faster healing.
- Superior Hemostasis – The laser quickly coagulates blood, minimizing bleeding, ensuring a clear surgical field, and shortening the overall procedure time.
Laser Treatment Frenectomy Before and After

Postoperative Recovery
- Cold Compress – Apply ice packs for 10 minutes to reduce swelling.
- Dietary Guidelines – Stick to a liquid diet for the first 24 hours; avoid hot drinks and spicy foods.
Oral Hygiene
- Rinse with saline solution three times daily.
- Avoid alcohol-based mouthwashes to prevent irritation.
Pain Management
- Use NSAIDs (e.g., ibuprofen) as needed.
- For children, acetaminophen is the preferred option.
Functional Training
- Start tongue stretching exercises 48 hours post-surgery (e.g., licking the upper lip) to aid functional recovery.
Clinical Outcomes
- A multicenter study reported a 98.2% complete healing rate with semiconductor laser procedures.
- Average healing time: 7–10 days (compared to 14 days with traditional surgery).
- Postoperative bleeding rate: <1%, significantly lower than the 8–12% reported for conventional surgery (AAPD 2023 guidelines).
Complication Management
- Scar Contracture – Rare occurrence (0.5% incidence rate).
- Revision Surgery – Only 0.2% of cases require a secondary procedure.
Diode Laser Treatment VS Traditional Surgical Methods
| Comparison Criteria | Traditional Surgery (Scalpel) | Diode Laser | Evidence & Clinical Data |
|---|---|---|---|
| Surgical Trauma | Requires mucosal and fibrous tissue incision, larger wound area, risk of damaging surrounding blood vessels/nerves. | Non-contact precise cutting, millimeter-level incision, preserves healthy tissue, minimizes mechanical trauma. | Laser reduces wound area by 60% and scar formation rate to 12% compared to traditional methods. |
| Intraoperative Blood Loss | Relies on hemostatic forceps or electrocautery, average blood loss: 8-12ml. | Simultaneous capillary sealing with laser, blood loss <5ml, often eliminating additional hemostasis. | Studies show 85% reduction in blood loss with laser versus traditional methods.¹ |
| Postoperative Recovery Time | Requires sutures, healing time ~14 days, suture removal may cause secondary pain. | Suture-free natural healing, average healing time: 7-10 days (children: ≤7 days). | Laser group’s pain scores (VAS) reduced by 40% within 3 days post-op.² |
| Complication Risk | Infection rate: 5%-8%, higher risk of scar contracture (~35%). | Laser sterilization lowers infection rate to <1%, scar formation rate: 0.5%-12%. | AAPD guidelines recommend lasers for pediatric procedures to reduce complications. |
| Anesthesia Requirement | Requires local infiltration anesthesia (with epinephrine), low compliance in children. | Topical anesthesia (e.g., 2% lidocaine gel) suffices, higher pediatric tolerance. | 85% of pediatric laser patients show no intraoperative distress. |
| Indication Scope | Suitable for thick fibrous frenums but limited in narrow spaces (e.g., small oral cavities). | Effective for thin-to-moderate frenums, precise excision of abnormal attachments, ideal for infants and complex anatomy. | Laser success rate for ankyloglossia correction: 98.2%.³ |
| Long-Term Functional Improvement | Higher recurrence risk (3%-5%) due to scar adhesion, requiring secondary surgery. | Restores near-normal tissue physiology, speech improvement rate >90%. | 5-year follow-up shows 15% higher speech correction success with laser. |
| Cost-Effectiveness | Lower equipment costs and procedure fees. | Higher initial equipment costs but long-term savings (reduced follow-ups/complication management). | Comprehensive analysis shows 20% lower 5-year total costs with laser. |
Conclusion
Diode laser dentistry , with its three core advantages—minimally invasive nature, precision hemostasis, and accelerated recovery —is redefining the clinical standards for lingual and labial frenectomies. Compared to traditional surgical methods, laser technology significantly reduces intraoperative bleeding (<5 mL), postoperative pain (40% lower VAS scores), and complication risks (infection rate <1%), while shortening healing time to 7–10 days. For pediatric patients, its compatibility with topical anesthesia enhances treatment compliance, achieving over 90% parental satisfaction.
As modern dental practitioners, adopting diode lasers is not just a technological upgrade but a strategic move to elevate patient experiences and clinic competitiveness. We urge professionals to embrace this innovation, delivering safer, more comfortable oral care through precise and efficient protocols.
Why choose lasers? Supported by clinical evidence and authoritative guidelines (e.g., AAPD recommendations), diode lasers have emerged as the gold standard for frenectomies. Their minimally invasive, precise, and efficient nature makes them ideal for children, patients with coagulation disorders, or those with heightened pain sensitivity.
References
-
Pediatric Compliance & Anesthesia: "Reduced Need of Infiltration Anesthesia Accompanied With Other Positive Outcomes in Diode Laser Application for Frenectomy in Children." National Center for Biotechnology Information (NCBI). View on PubMed
-
Comparative Efficacy: "A Comparative Study of The Results of Conventional Surgery and Diode Laser in Maxillary Labial Frenectomy: A Randomized Clinical Trial." National Center for Biotechnology Information (NCBI). View on PubMed
-
Functional Recovery (Ankyloglossia): "Lingual frenectomy: functional evaluation and new therapeutical approach." View on PubMed